For U.S. Healthcare Professionals

OPSUMIT® (macitentan) was studied in SERAPHIN, the largest long-term, outcomes-based pivotal trial of an ERA in PAH1
Long-term outcomes data in both monotherapy AND combination therapy1,2
Trial design1,2:
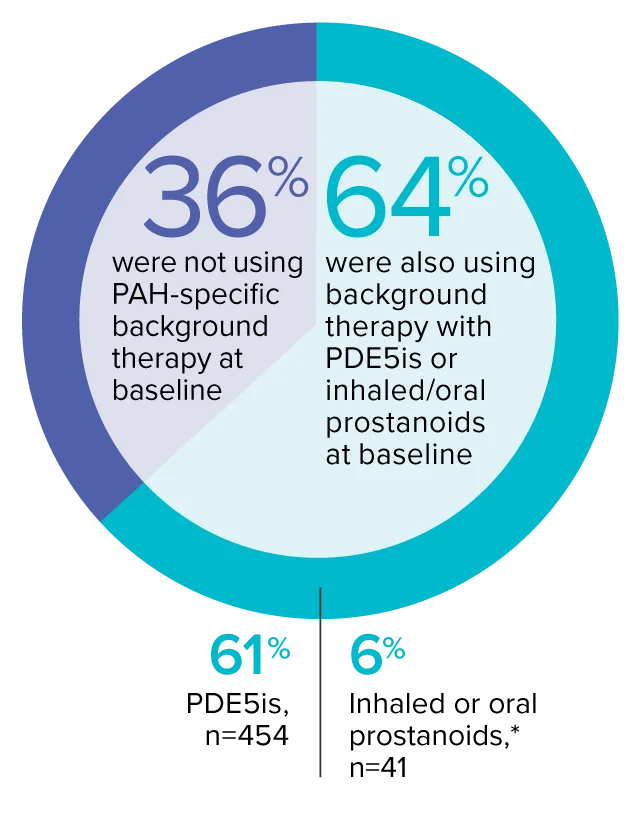
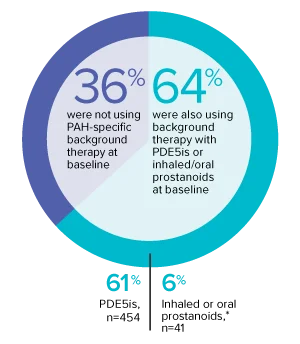
The effect of OPSUMIT® on disease progression in patients with PAH (WHO Group I) was studied in SERAPHIN, a large (N=742), event-driven, multicenter, long-term (average treatment duration 2 years), randomized, double-blind, placebo-controlled phase 3 trial. At study baseline, 36% of patients were not using PAH-specific background therapy and 64% were using stable background therapy for at least 3 months with PDE5 inhibitors or inhaled/oral prostanoids.*
Trial demographics1,3:
- Patients had predominantly WHO FC II (52%) and FC III (46%) symptoms
- Etiologies included IPAH/HPAH (57%), PAH-CTD (31%), PAH-CHD with repaired shunts (8%), PAH associated with drugs and toxins (3%), and PAH-HIV (1%)
- Mean patient age was 46 years, and 77% of patients were female
- 25% of patients were recently diagnosed (<6 months) and 75% were previously diagnosed (≥6 months)
Trial demographics1
742
Patients were randomized
Macitentan 3 mg is not
an approved dose.
Monotherapy and
combination therapy1,3
*Patients were treated with OPSUMIT® monotherapy or in combination with phosphodiesterase type 5 inhibitors or inhaled prostanoids.1
REPAIR study
EXPLORE ANALYSIS7-Year Data
EXPLORE ANALYSISSERAPHIN: Primary endpoint in overall study population†
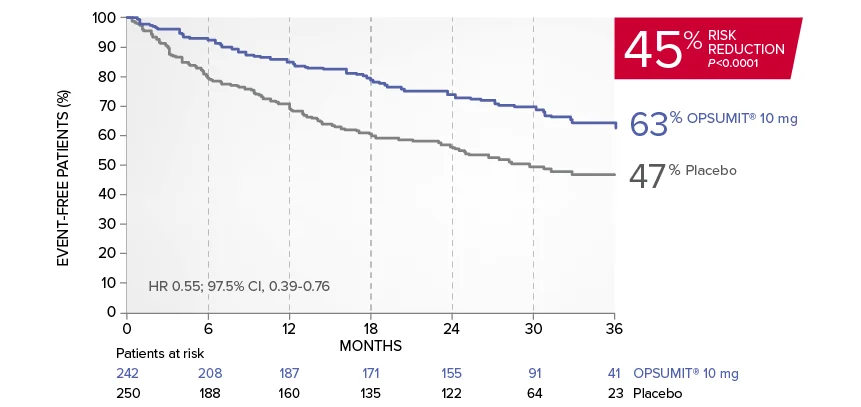
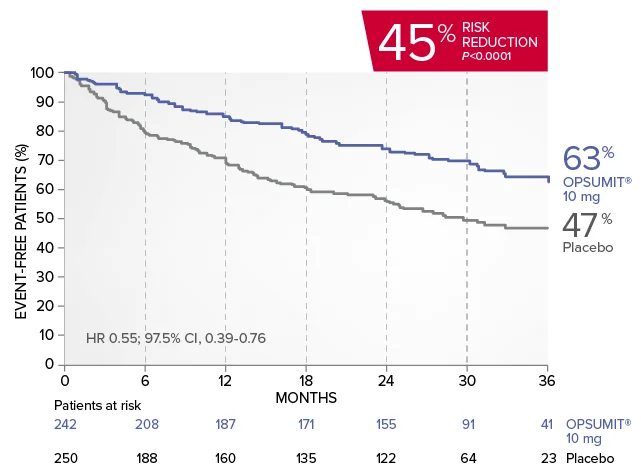
OPSUMIT® (macitentan) significantly reduced the risk of disease progression by 45% vs placebo1
The primary endpoint in the SERAPHIN trial was time to the first occurrence of death, a significant morbidity event, defined as atrial septostomy, lung transplantation, initiation of IV or SC prostanoids, or clinical worsening of PAH (defined as all of the following: a sustained ≥15% decrease from baseline in 6MWD,‡ worsening of PAH symptoms,§ and need for additional PAH treatment) during double-blind treatment plus 7 days.1,2
Kaplan-Meier estimates of risk of first primary endpoint event in SERAPHIN1,2
Summary of primary endpoint events1
| OPSUMIT® 10 mg (n=242), n (%) |
Placebo (n=250), n (%) |
|
|---|---|---|
| Patients with a primary endpoint event‖ | 76 (31.4) | 116 (46.4) |
| Component as first event | ||
| Worsening PAH | 59 (24.4) | 93 (37.2) |
| Death | 16 (6.6) | 17 (6.8) |
| Initiation of IV/SC prostanoids | 1 (0.4) | 6 (2.4) |
The beneficial effect of OPSUMIT® was primarily attributable to a reduction in clinical worsening events (defined as all of the following: a sustained ≥15% decrease from baseline in 6MWD,† worsening of PAH symptoms [a decline in WHO FC], and need for additional PAH treatment).
‖No patients experienced an event of lung transplantation or atrial septostomy in the placebo or OPSUMIT® 10 mg treatment groups.
OPSUMIT® can be started as monotherapy or in combination with PDE5 inhibitors or inhaled prostanoids.1*
*Patients were treated with OPSUMIT® monotherapy or in combination with phosphodiesterase type 5 inhibitors or inhaled prostanoids.1
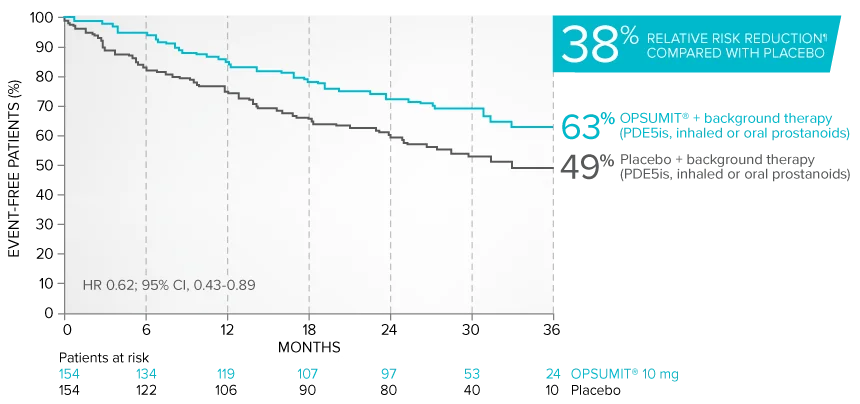
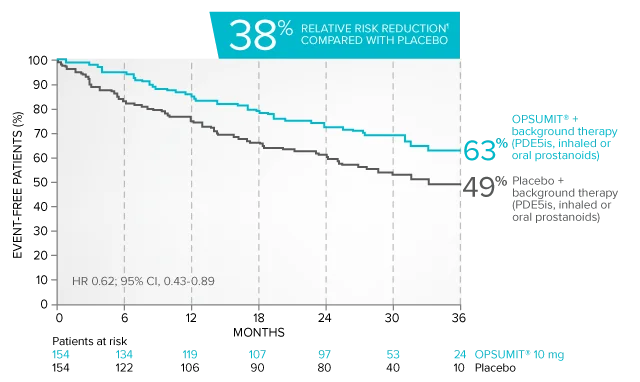
Combination therapy exploratory subgroup analysis in SERAPHIN trial
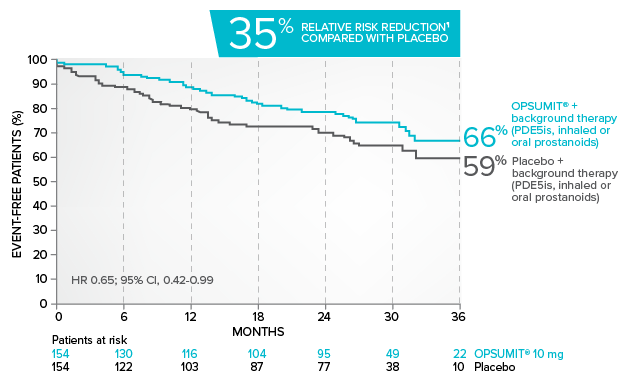
Kaplan-Meier estimates of risk of primary endpoint event when OPSUMIT® was added to stable PAH-specific background therapy1,3
At baseline, 64% of enrolled patients were treated with a stable dose of PAH-specific background therapy (61% PDE5 inhibitors; 6% inhaled or oral prostanoids).1*
*Patients were treated with OPSUMIT® monotherapy or in combination with phosphodiesterase type 5 inhibitors or inhaled prostanoids.1
Kaplan-Meier estimates of risk of first primary endpoint event1,3,4
¶Not adjusted for multiplicity.
Summary of primary endpoint events in patients treated with PAH-specific background therapy4
| OPSUMIT® 10 mg (n=154), n (%) |
Placebo (n=154), n (%) |
|
|---|---|---|
| Patients with a primary endpoint event‖ | 50 (32.5) | 68 (44.2) |
| Component as first event | ||
| Worsening PAH | 39 (25.3) | 58 (37.7) |
| Death | 10 (6.5) | 6 (3.9) |
| Initiation of IV/SC prostanoids | 1 (0.6) | 4 (2.6) |
‖No patients experienced an event of lung transplantation or atrial septostomy in the placebo or OPSUMIT® 10 mg treatment groups.
Common adverse reactions in the combination therapy exploratory subgroup5#
| OPSUMIT® 10 mg n=154 |
Placebo n=153 |
|
|---|---|---|
| Anemia | 16.2% | 4.6% |
| Nasopharyngitis | 11.0% | 10.5% |
| Bronchitis | 11.0% | 5.9% |
| Headache | 13.6% | 10.5% |
| Diarrhea | 13.0% | 9.8% |
#More frequent than placebo by ≥3%.
Combination therapy exploratory subgroup safety2,5
- The safety profile of OPSUMIT® as part of a combination therapy regimen was consistent with that of OPSUMIT® in the overall SERAPHIN population
- The incidence of peripheral edema, a known ERA-related adverse event, was similar in OPSUMIT®- and placebo-treated patients receiving background therapy (19.5% and 23.5%, respectively)
- Treatment discontinuations due to adverse events in patients receiving background therapy were similar in those receiving OPSUMIT® and those receiving placebo (9.1% and 11.8%, respectively)
Looking for patient enrollment resources?
Enroll PatientsSERAPHIN PAH-related hospitalization results
View the DataPAH-related hospitalization
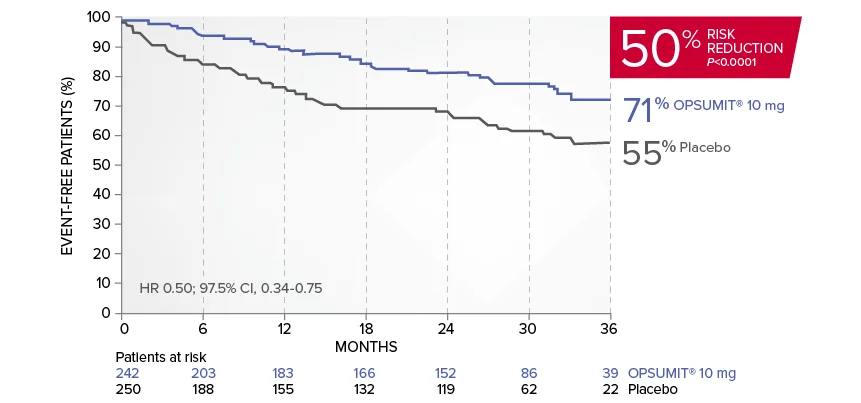
OPSUMIT® (macitentan) reduced the risk of PAH-related hospitalization1,2
A key secondary endpoint in SERAPHIN was death due to PAH or PAH-related hospitalization.
There was a 50% reduction in the risk of PAH-related hospitalization vs placebo in the overall population.†
Kaplan-Meier estimates of risk of first key secondary endpoint event1,2
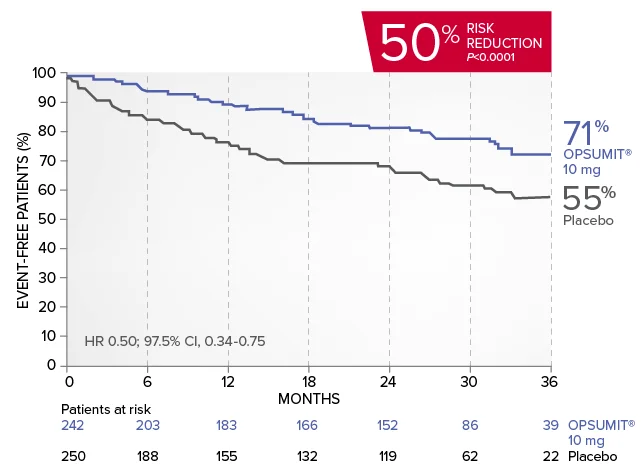
Summary of death due to PAH and hospitalization due to PAH1,2
| OPSUMIT® 10 mg (n=242), n (%) |
Placebo (n=250), n (%) |
|
|---|---|---|
| Death due to PAH or hospitalization for PAH | 50 (20.7) | 84 (33.6) |
| Component as first event | ||
| Death due to PAH | 5 (2.1) | 5 (2.0) |
| Hospitalization for PAH | 45 (18.6) | 79 (31.6) |
Exploratory subgroup analysis: Combination therapy results
Kaplan-Meier estimates of risk of first key secondary endpoint event when OPSUMIT® was added to stable PAH-specific background therapy6
- At baseline, 64% of enrolled patients were treated with a stable dose of PAH-specific background therapy (61% PDE5 inhibitors; 6% inhaled or oral prostanoids). Patients were treated with OPSUMIT® monotherapy or in combination with phosphodiesterase type 5 inhibitors or inhaled prostanoids.1
Kaplan-Meier estimates of risk of first key secondary endpoint event6
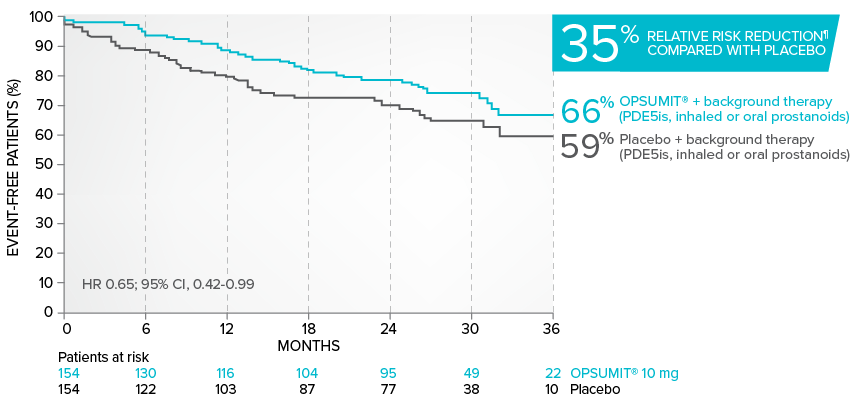
Summary of death due to PAH and hospitalization due to PAH6
| OPSUMIT® 10 mg (n=154), n (%) |
Placebo (n=154), n (%) |
|
|---|---|---|
| Death due to PAH or hospitalization for PAH | 37 (24.0) | 49 (31.8) |
| Component as first event | ||
| Death due to PAH | 2 (1.3) | 2 (1.3) |
| Hospitalization for PAH | 35 (22.7) | 47 (30.5) |
Common adverse reactions in the combination therapy exploratory subgroup5#
| OPSUMIT® 10 mg n=154 |
Placebo n=153 |
|
|---|---|---|
| Anemia | 16.2% | 4.6% |
| Nasopharyngitis | 11.0% | 10.5% |
| Bronchitis | 11.0% | 5.9% |
| Headache | 13.6% | 10.5% |
| Diarrhea | 13.0% | 9.8% |
#More frequent than placebo by ≥3%.
Combination therapy exploratory subgroup safety2,5,6
- The safety profile of OPSUMIT® as part of a combination therapy regimen was consistent with that of OPSUMIT® in the overall SERAPHIN population
- The incidence of peripheral edema, a known ERA-related adverse event, was similar in OPSUMIT®- and placebo-treated patients receiving background therapy (19.5% and 23.5%, respectively)
- Treatment discontinuations due to adverse events in patients receiving background therapy were similar in those receiving OPSUMIT® and those receiving placebo (9.1% and 11.8%, respectively)
†All randomized patients.
¶Not adjusted for multiplicity.
Looking for patient enrollment resources?
Enroll PatientsOPSUMIT® (macitentan): Additional endpoints from the SERAPHIN trial
SERAPHIN included secondary and exploratory endpoints from baseline to Month 6
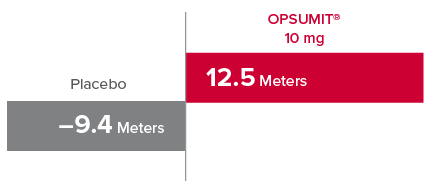
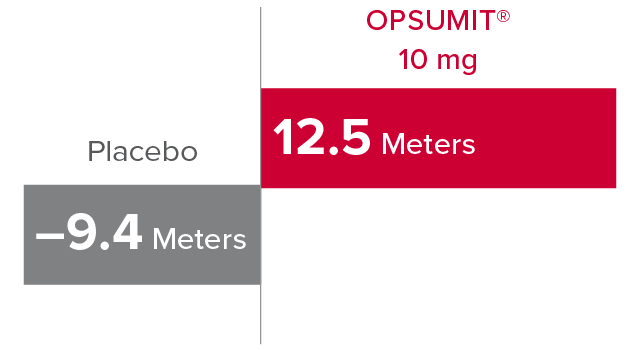
Change from baseline in 6MWD at Month 61,2
At Month 6, 6MWD had increased by a mean of 12.5 m in the group receiving OPSUMIT® 10 mg (n=242); 6MWD decreased by a mean of 9.4 m in the placebo group (n=249) (placebo-corrected mean increase of 22.0 m; 97.5% CI, 3.0-41.0; P=0.0078).
Change in 6MWD at Month 6
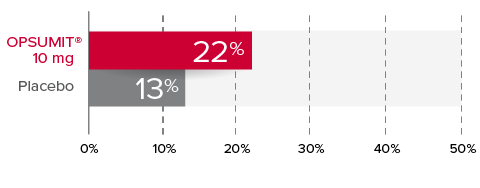
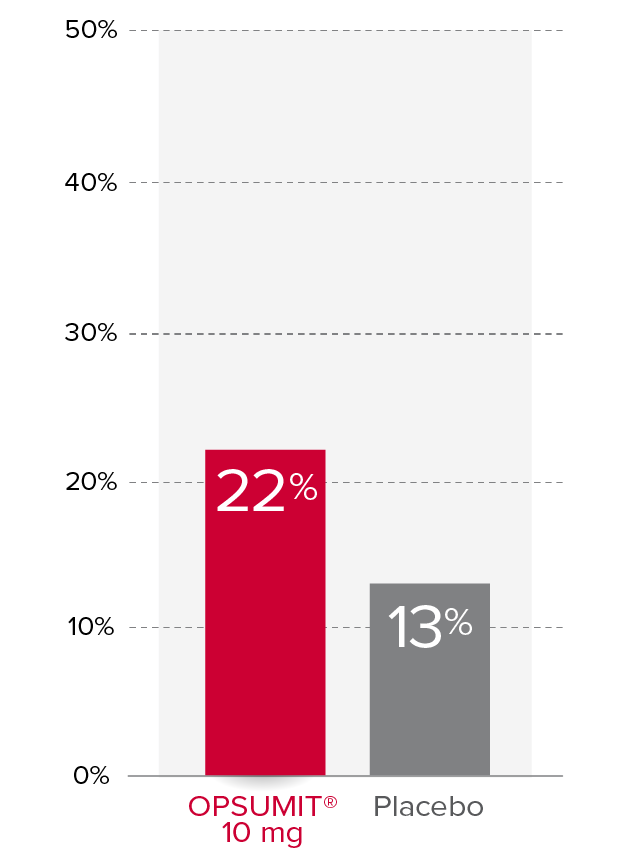
Changes from baseline in WHO FC1,2
At Month 6, 22% of patients in the OPSUMIT® 10 mg group (n=242) experienced improvement of at least 1 WHO FC vs 13% of patients in the placebo group (n=249) P=0.006.
% Patients with improvement of at least
1 WHO
FC at
Month 6
Change from baseline in measures of hemodynamics at Month 61,7,8
Exploratory hemodynamic substudy within SERAPHIN (OPSUMIT®: n=57, placebo: n=67).
PVR¶
37%
median reduction
in PVR vs
placebo
(95% CI, 22-49)
Mean PVR at BL
for OPSUMIT®:
924 ± 532
dyn•sec/cm**
Cardiac Index¶
0.6
L/min/m2
median increase
in cardiac index vs placebo
(95% CI, 0.3-0.9)
Mean cardiac index
at BL for OPSUMIT®:
2.55 ± 0.85
L/min/m2**
¶Not adjusted for multiplicity.
**Plus-minus values are mean ± standard deviation.
SERAPHIN PAH-related hospitalization results
View the DataView SERAPHIN PAH-CTD subgroup data
See the DataPAH associated with connective tissue disease (PAH-CTD)
PAH: A potential complication of CTD affecting up to approximately 1 in 10 patients9
PAH is a well-known complication in some patients with CTD10:
- PAH affects approximately 3% to 13% of patients with CTD and 5% to 12% of patients with systemic sclerosis (SSc)9,11
- Patients with PAH-SSc have a worse prognosis than most other PAH-associated disease populations12
Exploratory subgroup analysis: Disease progression in patients with PAH-CTD
Overall, in SERAPHIN, OPSUMIT® (macitentan) reduced the risk of disease progression by 45% vs placebo (HR 0.55; 97.5% CI, 0.39-0.76; P<0.0001).1 In the SERAPHIN trial, 31% of the overall patient population had PAH-CTD.1
POST HOC ANALYSIS: Time to first disease progression event in patients with PAH-CTD13,14
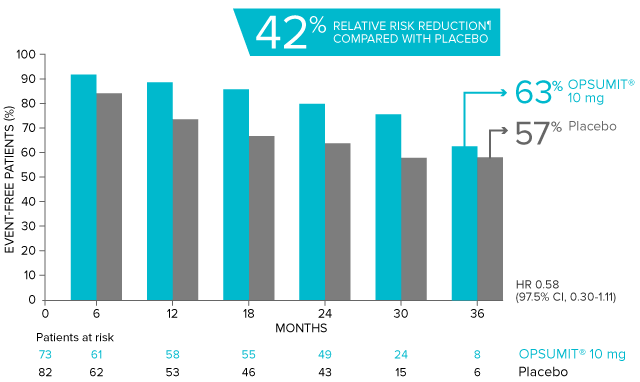
Summary of primary endpoint events in patients with PAH-CTD13
| OPSUMIT® 10 mg (n=73), n (%) |
Placebo (n=82), n (%) |
|
|---|---|---|
| Patients with a primary endpoint event* | 20 (27.4) | 31 (37.8) |
| Component as first event | ||
| Worsening PAH | 16 (21.9) | 25 (30.5) |
| Death | 3 (4.1) | 5 (6.1) |
| Initiation of IV/SC prostanoids | 1 (1.4) | 1 (1.2) |
*No patients experienced an event of lung transplantation or atrial septostomy in the placebo or OPSUMIT® 10 mg treatment groups.
Differences in PAH-CTD subgroup baseline characteristics compared with SERAPHIN overall population2,13
- Larger percentage of female patients (92% vs 76.5%)
- Older average age (49.7 years vs 45.6 years)
- Larger percentage of patients with WHO FC II symptoms (58.5% vs 52.4%)
- Lower percentage of patients with WHO FC Ill symptoms (39.3% vs 45.6%)
- Shorter time from diagnosis (mean 2.0 years vs 2.7 years)
Adverse reactions in the PAH-CTD subgroup different from the overall population13††
| OPSUMIT® 10 mg n=73 |
Placebo n=82 |
|
|---|---|---|
| Upper respiratory tract infection | 23.3% | 13.4% |
| Urinary tract infection | 12.3% | 6.1% |
| Skin ulcer | 9.6% | 3.7% |
| Sinusitis | 6.8% | 1.2% |
| Lower respiratory tract infection | 5.5% | 1.2% |
| Nausea | 8.2% | 4.9% |
††Only adverse reactions occurring ≥3% on OPSUMIT® compared with placebo and placebo-corrected difference of ≥3% in the PAH-CTD subgroup vs the overall population are shown here.
Eight (9.8%) patients receiving placebo and 8 (11.0%) patients receiving OPSUMIT® 10 mg in the PAH-CTD subgroup discontinued treatment due to adverse reactions, compared with approximately 11% for both the placebo and OPSUMIT® in the overall population.2,13
Exploratory subgroup analysis: PAH-related hospitalization
Overall, in SERAPHIN, OPSUMIT® reduced the risk of PAH-related hospitalization by 50% vs placebo (HR 0.50; 97.5% CI, 0.34-0.75; P<0.0001).1
POST HOC ANALYSIS: Time to PAH-related
death or
hospitalization in patients with PAH-CTD13,15
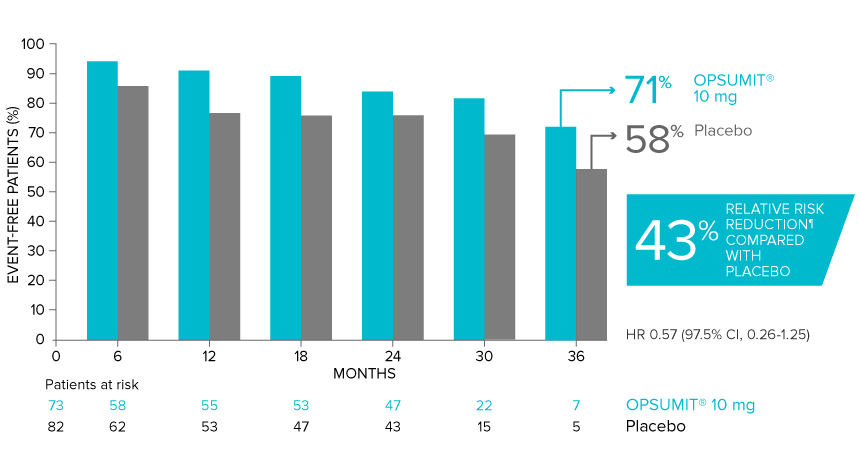
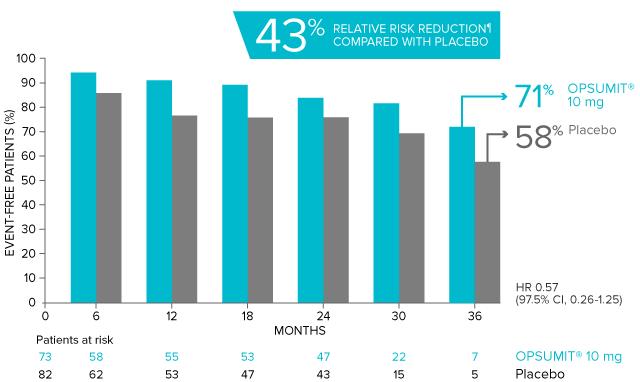
PAH-CTD Subgroup: Summary of death due to PAH and hospitalization due to PAH13
| OPSUMIT® 10 mg (n=73), n (%) |
Placebo (n=82), n (%) |
|
|---|---|---|
| Death due to PAH or hospitalization for PAH | 13 (17.8) | 22 (26.8) |
| Component as first event | ||
| Death due to PAH | 1 (1.4) | 1 (1.2) |
| Hospitalization for PAH | 12 (16.4) | 21 (25.6) |
Looking for patient enrollment resources?
Enroll PatientsSERAPHIN PAH-related hospitalization results
View the Data‡Confirmed by a 6-minute walk test performed on a different day within 2 weeks.
§Worsening of PAH included at least one of the following: Advancing to a higher FC from baseline (or no change in WHO FC IV) and signs of right heart failure that does not respond to oral diuretic treatment.
¶Not adjusted for multiplicity.
#More frequent than placebo by ≥3%.
**Plus-minus values are mean ± standard deviation.
6MWD=6-minute walk distance; BL=baseline; CI=confidence interval; CTD=connective tissue disease; ERA=endothelin receptor antagonist; FC=Functional Class; HPAH=heritable PAH; HR=hazard ratio; IPAH=idiopathic PAH; IV=intravenous; PAH=pulmonary arterial hypertension; PAH-CHD=PAH associated with congenital heart disease; PAH-CTD=PAH associated with connective tissue disease; PAH-HIV=PAH associated with human immunodeficiency virus; PAH-SSc=PAH associated with systemic sclerosis; PDE5i=phosphodiesterase type 5 inhibitor; PVR=pulmonary vascular resistance; SC=subcutaneous; SERAPHIN=Study with an Endothelin Receptor Antagonist in Pulmonary Arterial Hypertension to Improve CliNical Outcome; WHO=World Health Organization.
This site is intended for U.S.
healthcare professionals

You are now leaving OpsumitHCP.com
Clicking CONTINUE below will take you to the selected site, the content for which Johnson & Johnson is not responsible and to which this Privacy Policy does not apply. We encourage you to read the Privacy Policy of every online service you visit.
You are now leaving OpsumitHCP.com
Clicking CONTINUE below will take you to the selected site, the content for which Johnson & Johnson is not responsible and to which this Privacy Policy does not apply. We encourage you to read the Privacy Policy of every online service you visit.
You are now leaving OpsumitHCP.com
Clicking CONTINUE below will take you to the selected site, the content for which Johnson & Johnson is not responsible and to which this Privacy Policy does not apply. We encourage you to read the Privacy Policy of every online service you visit.
You are now leaving OpsumitHCP.com
By clicking on “Continue” below, you will leave OpsumitHCP.com and be directed to the Janssen CarePath site.
You are now leaving OpsumitHCP.com
By clicking on “Continue” below, you will leave OpsumitHCP.com and be directed to the site for iAssist registration.
You are now leaving OpsumitHCP.com
Clicking CONTINUE below will take you to the selected site, the content for which Johnson & Johnson is not responsible and to which this Privacy Policy does not apply. We encourage you to read the Privacy Policy of every online service you visit.
You are now leaving OpsumitHCP.com
Clicking CONTINUE below will take you to the selected site, the content for which Johnson & Johnson is not responsible and to which this Privacy Policy does not apply. We encourage you to read the Privacy Policy of every online service you visit.
You are now leaving OpsumitHCP.com
Clicking CONTINUE below will take you to the selected site, the content for which Johnson & Johnson is not responsible and to which this Privacy Policy does not apply. We encourage you to read the Privacy Policy of every online service you visit.
You are now leaving OpsumitHCP.com
Clicking CONTINUE below will take you to the selected site, the content for which Johnson & Johnson is not responsible and to which this Privacy Policy does not apply. We encourage you to read the Privacy Policy of every online service you visit.
You are now leaving OpsumitHCP.com
Clicking CONTINUE below will take you to the selected site, the content for which Johnson & Johnson is not responsible and to which this Privacy Policy does not apply. We encourage you to read the Privacy Policy of every online service you visit.